Our airwaves, like our organs and limbs, are suffocated by expanding flab. Fat dominates the news. In the last month alone, the National Obesity Forum suggested that regular weight checks should be compulsory; a European court ruled that obesity is a disability after the sacking of a 25-stone Danish child-minder; and the chief executive of NHS England called the same ruling "daft", declaring war on obesity after a study found that only Hungary has fatter adults than the UK. Queensland, meanwhile, declared an "obesity state of emergency"; the Saudis organised an anti-obesity run; federal regulators in the US approved an appetite-suppressing implant; a Canadian study linked a type of serotonin with obesity; and a Harvard team found two compounds that turn "bad" white fat cells into "good" brown fat ones.
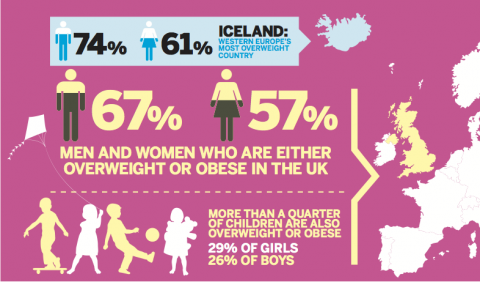
The Western world is preoccupied with obesity, and rightly so, because the statistics of our expanding girths are shocking by any measure. Twenty-five per cent of citizens in most Westernised countries, including the UK, are now obese; and about half of the population is overweight. The problem is so immense that lifespans, it is predicted, may begin falling, rather than rising, for the first time in history.
Even more worryingly, it is not so much the length of life as its quality that is affected by fat. Being obese means we are more likely to suffer from mobility and joint problems such as aching knees, type 2 diabetes, heart disease, and certain cancers – as well as social stigma and diminished mental health.
A predisposition for obesity, alongside a fondness for smoking and drinking (exacerbated by its pervasive association with the underclass) has been condemned in the court of public opinion as a moral weakness. It is an issue for those who lack self-control or the ability to help themselves; in other words, an issue only for those without any sense of personal dignity or responsibility.
In the course of writing this piece I spoke to several intelligent, usually sympathetic, types who displayed the near-anger, disgust even, that the educated classes feel for the "feckless fat". "They just need to eat less," people say.
While this is true, things aren't quite that simple. For a start, less of what? Once it was saturated fats; now sugar is the fashionable smoking gun. Some, reductively, argue that a sugar tax would bring an end to the problem. Certainly sugary drinks, from soda to fruit juice, are particularly unhelpful because though they are calorific they do not alleviate hunger. In obesity terms, this is toxic.
But politicians are reluctant to level taxes on foodstuffs – partly because they don't want to annoy the food-and-drinks lobby, a significant player in any economy, and partly because such taxes always disproportionately penalise the poor. In Denmark and New York, fiscal measures didn't work, and were shelved.
So while everyone knows there is a problem, many of the answers are controversial because, in the British mind, the flip-side of personal responsibility is personal liberty. While we must have the freedom to eat whatever we like, anyone who chooses to abuse that right is weak-willed, greedy and self-destructive.
And so it is that complications from type 2 diabetes, a disease largely brought on by obesity, are costing the NHS £1.5m an hour – 10% of its annual budget. Is the problem too big to stall?
The Beginning of Fat
Let's wind back a little see how we arrived at this mess. In any society, there have always been severely obese people. The Venus of Willendorf, a statuette of a very roly-poly female figure found in rural Austria, dates from before 25,000 BC; Hippocrates wrote about obesity in the fourth century BC. In 1700, as England became more prosperous and its food supplies more reliable, Thomas Short wrote A Discourse Concerning the Causes and Effects of Corpulency. At the time, though, the condition was a rarity.
It is only since the Second World War that the march of fat has accelerated. Coincident with our moving in from the fields and working in increasingly sedentary office jobs, food supplies have become more plentiful, cheaper, and laden with fat and sugar. Just as our calorific output went drastically down, our calorific input went drastically up.
Multiple environmental reasons have compounded the problem: the availability of calorie-laden, cheap, deliberately-addictive fast food; the reduction in exercise among urban children, fuelled by a rise in interest in computer games, a fear of letting children play outside, and scaled-back state-school sport; an increase in city living, and a concurrent rise in the use of public transport and takeaway food outlets; and the ever-more sophisticated marketing techniques of food companies. Even central heating has played its part – since we no longer shiver, we no longer have to move around as much to stay warm. Gyms, meanwhile, are a mixed blessing. Intensive exercise (unlike, say, working in the fields all day or walking everywhere) is unlikely to be sustained over time, and is subject to interruption by even mild injury. It is also likely to boost appetite.
So we hear the (often accurate) horror stories of the need for NHS beds to be doubled in size; of morgues with bodies too big for their fridges; of airline seats rebuilt to accommodate the large. Tabloids feature a gallery of grotesques: teenagers carried out of their houses by stretcher, men who are unable to leave theirs at all.
The severely obese have their own specific set of problems. But underneath these outliers there is a growing army: the overweight and less-severely obese, who are getting fatter and fatter, and less and less healthy.
In a world that, incredibly, has more overfed than underfed people in it, even the way we look at fat has changed. The problem of over-nutrition is so severe that those of ideal weight (between 18 and 25 on the BMI index) now look malnourished to us. Obesity is so prevalent we can't even see it straight.
Inventing the Fat Pill
In order to see what we're doing about this complicated problem, I went to visit Britain's war rooms in the fight on flab: the Wellcome Trust-Medical Research Council Institute of Metabolic Science in Cambridge. It's the vision of an affable, determined and imaginative Irishman, Professor Sir Stephen O'Rahilly.
The Institute opened in 2008 next to Addenbrooke's Hospital. On the ground floor there is a clinic for diabetic patients, – adult and paediatric – who often join trials. On the second floor, Professor Nick Wareham runs the public health department, looking at measures that might make a difference to the population at large. In January, he announced the results of a study of 334,000 people which showed the importance of exercise – 20 minutes a day cuts the risk of premature death by a third.
Meanwhile on the top two floors, Professor O'Rahilly's 19 principal investigators examine all manner of scientific angles on obesity: the specific genes involved; what happens in utero; the effect of circadian rhythms.
The bigger the problem, the greater the glory – and the riches – at stake for any person, or any company, who can produce the much-discussed miracle pill, the magic bullet that can make the world thin again.
It is no exaggeration to say that millions of lives and billions of pounds are at stake. There is a secretive global arms race under way to develop a cure, of which O'Rahilly is part and is probably, given his reputation, our best bet.
"Many people are trying to work on mimicking the effects of bariatric [gastric bypass] surgery through the use of medicines that a) mimic or enhance the effects of natural satiety hormones produced by the gut after food and/or b) enhance the amount of those natural hormones produced after food," he explains. He won't go into detail about his own trials, or even tell me which pharma company he's working with. While other global teams release enticing snippets that may or not may lead anywhere, this is not O'Rahilly's style.

The most effective surgery works by making people feel full. But such surgery is dangerous, expensive, and one-size-fits-all. A pill that can trick the brain into feeling full by elevating satiety hormones and thus sending it false messages from the gut – which, I sense from O'Rahilly's caginess, may not be that far off – will change everything. Only feeling full will stop us from eating, and if we can medically induce that, then we will have slayed the obesity dragon.
The other advantage of a pill over surgery, says O'Rahilly, is that is it can potentially be personalised. Clearly, half of Europe cannot have a bariatric procedure. But they could be given different combinations of hormones to stop them eating so much.
Such a pill would be a seminal breakthrough. O'Rahilly's team, though, are thorough, and there doesn't seem to be an angle on obesity that they're not investigating. His colleague, Dr Giles Yeo, says we tend to look at obesity in the wrong light. Rather than just condemning those who overeat, he says, we should be asking, "Why, exactly, do some people eat too much, when others don't?" Our environment plays its part, but how we eat is powerfully genetically determined, "because of how we got to today . . . all of us are programmed to survive long enough to reproduce. In order to survive that long you need to eat, and you need to survive. For the entire history of our existence as a living, breathing creature, too little food has been around, until the last 50 years. Pre-agriculture, in the Serengeti, we caught an antelope, brought it back and ate it because didn't know what would happen next – we would eat, and prepare for famine.'" In other words, our genes tell us – more loudly in some of us than in others – to eat whenever we can.
Fifty years, in context of genetics, is the blink of an eye; our bodies haven't yet adapted to our suddenly food-dense environment. As Yeo puts it, "our body frame has evolved to be lean" and is unable to adapt to our new habits. If we do become obese, our chances of getting heart disease and cancer, and dying early, rise. So there is now a catastrophic mismatch of our genes and our environment. Once, very few of us could overeat. Today in the West most of us can – we can all be Henry VIII now. Of course, this doesn't mean that everyone is fat – the less-hungry stay thin. Although in Serengeti terms, you could argue that the fat ones are more evolved. "Perhaps, back then, Kate Moss types would have been lion food," says Yeo.
The Genetic 'Crunch'
The genetic argument is not a popular one. Yeo tells a story of a man at a Cambridge college dinner pointing at him saying, "you are giving them a crutch." Yeo says, "If Mrs Smith, a 25-stone diabetic about to die, chooses to use heritability as a crutch, the only person who's going to suffer is her. But ignoring the role of genetics is helpful to no one."
As Yeo sees it, those who eat less aren't morally stronger, they are just people who don't feel like eating as much, just like those who feel like taking more exercise. O'Rahilly's team often looks at the extremes – the severely obese, and now the very underweight – not only to help them, but also because a study of the margins often yields clear insights into the more muddled mainstream.
Professor Sadaf Farooqi studies severely obese children. Although we are fatter because we take in more calories than we burn, what we choose to eat isn't always a rational decision. In children it is more complicated still, because it isn't always clear who is choosing what.
Farooqi reads me a recent email from a professor of endocrinology at Harvard. She writes that she "had her work cut out" with a piece from The New York Times in June titled, "In Britain's, Child's Weight Leads to Parents' Arrest". The parents of an 11-year-old boy in Norfolk, who weighed 210 pounds, had been arrested. "There is a massive failure of understanding when it comes to severe obesity," says Farooqi. Later, O'Rahilly tells me they have heard of children eating food straight from the freezer, and chewing on bin scraps, because they feel extreme hunger.

The idea that you might take a child away from its parents because of its size is a "travesty", Farooqi says, because, ironically, the more severely obese the child, the more likely it is that genes are playing a powerful part. She has seen children from war-torn Liberia and rural Pakistan who are severely obese when you might expect them to be malnourished. There is no way, she says, that the parents are to blame in these cases; who could possibly get a three-year-old to 36 kilos? As all parents know, young children eat what they want to eat and nothing else.She is currently working on a study involving a disorder that affects some 50,000 people in the UK (and over a million globally) and that may be able to remedy another defect in the brain concerning hunger and satiety. O'Rahilly's study on "extreme metabolic phenotypes" (people with rare genetic defects) led him to identify children with a congenital leptin deficiency. Leptin is a hormone that causes people to feel full after eating; when he treated the children with doses of the missing hormone, even those who were nearly wheelchair-bound returned to a normal weight. That was a breakthrough; but leptin, frustratingly, proved ineffective for all but the most chronically deficient. It wasn't quite the magic bullet.
Farooqi finds it frightening that society is so judgemental. In the case of the three-year-old in Manchester, she identified a genetic problem. "I never realised I'd be getting involved in these disputes, but I want to help the patients, partly because of the social stigma. Public awareness means that people are confusing the population problem with the more unusual problem of severe obesity. People think parents must be taking toddlers to McDonald's 10 times a day. But it's often a biological problem. I don't think children should ever be taken away from their parents for weight reasons alone," she says.
On the other hand, obese parents do often have obese children. Farooqi estimates the genetic component at 40–70%. In other words, we inherit much of our propensity to fat, our appetite and our metabolism. More and more genetic factors are being identified. O'Rahilly is currently excited about Labrador dogs; with the Department of Veterinary Medicine, they have worked out why some Labradors are hungrier than others. This may lead to treatment for flabby Labs and, possibly, information on the fight against fat in the human population (insulin was first identified in dogs, and research is often performed on mice – leptin, for example, was first identified in the rodents).
The Price of Being Thin
If O'Rahilly had to point the finger at anything that got us into this, it would be food transportation. Never in history has "so little percentage of income been needed to buy so much food," he says. There's the rise of discount retailers like Aldi and Lidl, and portion expansion – croissants the size of boomerangs; buckets of popcorn and Coke. As his colleague Yeo says, if we could wind the clock back to 1950, obesity would go away, but we can't, so we have to find a way to deal with it.
The cure will be multifaceted, just as it has been for high blood pressure. O'Rahilly draws me a graph: like blood pressure, obesity has a normal range and a rather arbitrary cut-off point at which normal tips into excessive. Blood pressure is now manageable because of an awareness of the dangers of salt and an accompanying reduction in its consumption, and because of drugs such as statins that control it. Hospitals were once full of those suffering from the effects of hypertension, such as strokes – but no longer. The hope is that through a variety of environmental and pharmaceutical measures, obesity, too, will become manageable, a crisis of the past.

The key might be in genetic treatment, or otherwise in a magic pill that mimics the effects of gastric bypass surgery. A team from Barts and the London School of Medicine and Dentistry, for example, announced recently that they were five years away from producing one. "Bands and balloons don't really work and shouldn't be heaped together with other surgery," says O'Rahilly, "a stomach bypass is effective because as the food goes into the intestine lower down, the brain is tricked into thinking it's full. But it is surgery, and it is expensive."
O'Rahilly, working alongside pharmaceutical companies, sees his team as a kind of military intelligence, and the companies as their weaponry. There have been other pills in the past: safe ones that weren't effective; effective ones that weren't safe. His promising early-phase trials have a clear aim: that high body-weight eventually becomes, like high blood pressure, "easily, cheaply treatable, and no longer life-threatening."
Like the rest of his team, he is non-judgemental and intensely sympathetic to the obese. "Thin people are not morally superior. They are less prone to obesity, and those who are unlucky are not feckless. They are biologically different. I want to see what we can tweak under the bonnet."
It's not a straightforward task. "Unlike cancer – when people who know they might die will take anything – obesity kills you very slowly so we can only use safe agents." Obesity studies struggle with funding because of the moral angle – "an obese man eventually dies of a heart attack and his widow gives money to a heart charity," says O'Rahilly drily.
He thinks in spite of data that show sharp acceleration in recent years, there is also some evidence that obesity is levelling out, particularly among children – that it won't continue rising to a point where we are all obese.
Governments are taking notice. O'Rahilly broadly supports a sugar tax, although he thinks that, ideally, food companies will one day find that healthy food equals more profit.
The Sugar Demon
Some things are simple. When sugary drinks are restricted in lunch boxes, studies show that weight falls. "It's not magic – it's just lowering calorie intake," says O'Rahilly. Sugary drinks are particularly dangerous because they are not filling – they're empty calories.
And as Yeo says, sugar has the power to distort the appetite: "people will have a dessert when they'd never have another portion of mashed potato."
O'Rahilly recently wrote that while glucose and fructose are equal in calories, and therefore equal in their ability to cause weight gain, fructose is worse for us because "it's handled differently in the body, especially the liver. As a consequence of this, high-fructose diets in rodents tend to cause high lipid levels in the blood, insulin resistance, high uric acid (the substance that precipitates out in joints when we get gout) and high blood pressure."
In conclusion, O'Rahilly wrote: "There is evidence that excessive consumption of fructose (found in sugar and in high-fructose corn syrup) is associated with a worsened metabolic state than excessive consumption of glucose, even though both forms of overconsumption can increase weight and fat stores to a similar amount. This provides further evidence that policies designed to discourage the ingestion of sweetened beverages would likely have a positive impact on public health."
So even within sugars, some calories are worse for your health than others. To complicate matters further, Professor Toni Vidal-Puig says it's not as simple as "fat equals bad, thin equals good".

All fat is not equal. Internal fat can be even more dangerous than the external kind. They are investigating why a 200kg man can be healthier than an 80kg one. "If his adipose tissue doesn't work as well then the fat will go to his muscles, heart and liver." This is part of O'Rahilly's second question (after that of what makes some people obese): why excess weight leads to illness and why, sometimes, it doesn't.
In another area of Vidal-Puig's studies lies, potentially, an amazingly simple fix. In spite of all the millions spent on diets, food and exercise, it may be that something as basic as temperature is the answer. We all have two types of fat, white and brown. White fat is inert and sits in deposits. Brown fat, which regulates babies' temperatures but is much harder to pinpoint in adults, can be activated to burn calories and generate heat.
Studies show that exposure to low temperatures may encourage white fat to behave like brown fat. So while central heating ensures we move less and burn fewer calories, it's possible that lower temperatures might increase the activity of brown fat, which will burn our calories for us. "It is indeed theoretically possible that if we all switched on our brown fat by living in colder ambient temperatures we might all expend more energy," says O'Rahilly.
It's a nice idea, he says, but so far there has not been sufficient study to show whether it's possible, or whether our bodies will compensate in other ways by making us eat more.
The Big Breakthrough
Scientists at the Stem Cell Institute at Harvard and Massachusetts General Hospital (one of the many teams in the world to have joined the race) announced before Christmas that they had identified two compounds that could turn "bad" white fat into "good" brown fat, in what is possibly a step towards their own version of that magic pill. One of the two compounds is already used to treat rheumatoid arthritis, but the team admits they are some way from their pill because the compounds concerned could damage the immune system.
Associate Professor Chad Cowan says, "If you administered them [the compounds] for a long time, the person taking them could become immune-compromised . . . The good news and bad news is that science is slow; just establishing proof of concept takes an enormous amount of time."
At the same time, another player – a team of researchers from Imperial College, London – identified an enzyme called glucokinase which could possibly be target for a new pill because it drives the craving for sugar in the brain.
"This is the first time anyone has discovered a system in the brain that responds to a specific nutrient, rather than energy intake in general. It suggests that when you're thinking about diet, you have to think about different nutrients, not just count calories," says James Gardiner of Imperial College, whose study was published in The Journal of Clinical Investigation. His tests on rats showed that boosting glucokinase activity caused the animals to consume glucose over normal food. If a pill could reverse this desire, sugar consumption would decrease.
Earlier this month, a report was published in Nature Medicine from researchers at the Salk Institute in La Jolla, California, claiming they had developed a drug that works like an "imaginary meal", which was shown to reduce obesity in mice. O'Rahilly says of the paper, "If we could fool those cells into thinking we have had a meal, that could be a way of reducing people's food intake to produce safe weight-loss. While these are interesting observations, only a modest percentage of drugs that seem effective in mice ever make it into the clinic for patients." So, in spite of the constant flow of exciting announcements, most of them, as yet, seem to be better news for rotund rodents than obese people.
Work in Cambridge isn't confined to O'Rahilly's team; Professor Nick Wareham, on the second floor, examines the population as whole. The causes of the obesity epidemic are not quite the same as the causes of obesity in individuals. Education and labelling, Wareham believes, can only go so far because we are not rational creatures. He wrote a paper recently in the British Medical Journal studying the importance of exposure to takeaway food: the more outlets, the higher the local bodyweight. That might sound obvious – but lined up with the fact that flat, spacious countries have more cyclists, a central point emerges: people are suggestible. They will do whatever is easiest. So we should perhaps look at changing the environment rather than just telling people to change their habits. "If I was forced to choose, diet matters the most," says Wareham, "But so does the environment and the infrastructure."
Somewhere between magic tablets, genetic studies, sugar taxes, cycle lanes, turning the central heating down, education and sympathy, O'Rahilly and Wareham, and others of their noble breed will, I hope, help cure us with kindness and ingenuity. Until then, the fat battle rages on.