The dangers of antibiotic-resistant bacteria have reached the pediatric ward. According to a new study, the number of hospitalized children in the U.S. infected with bacteria resistant to multiple types of antibiotic drugs surged between 2007 and 2015. The study is the first to confirm the extent of infections with multidrug-resistant (MDR) bacteria—superbugs, many experts call them—among children, and underscores the alarming proliferation of bacterial pathogens our medications no longer treat.
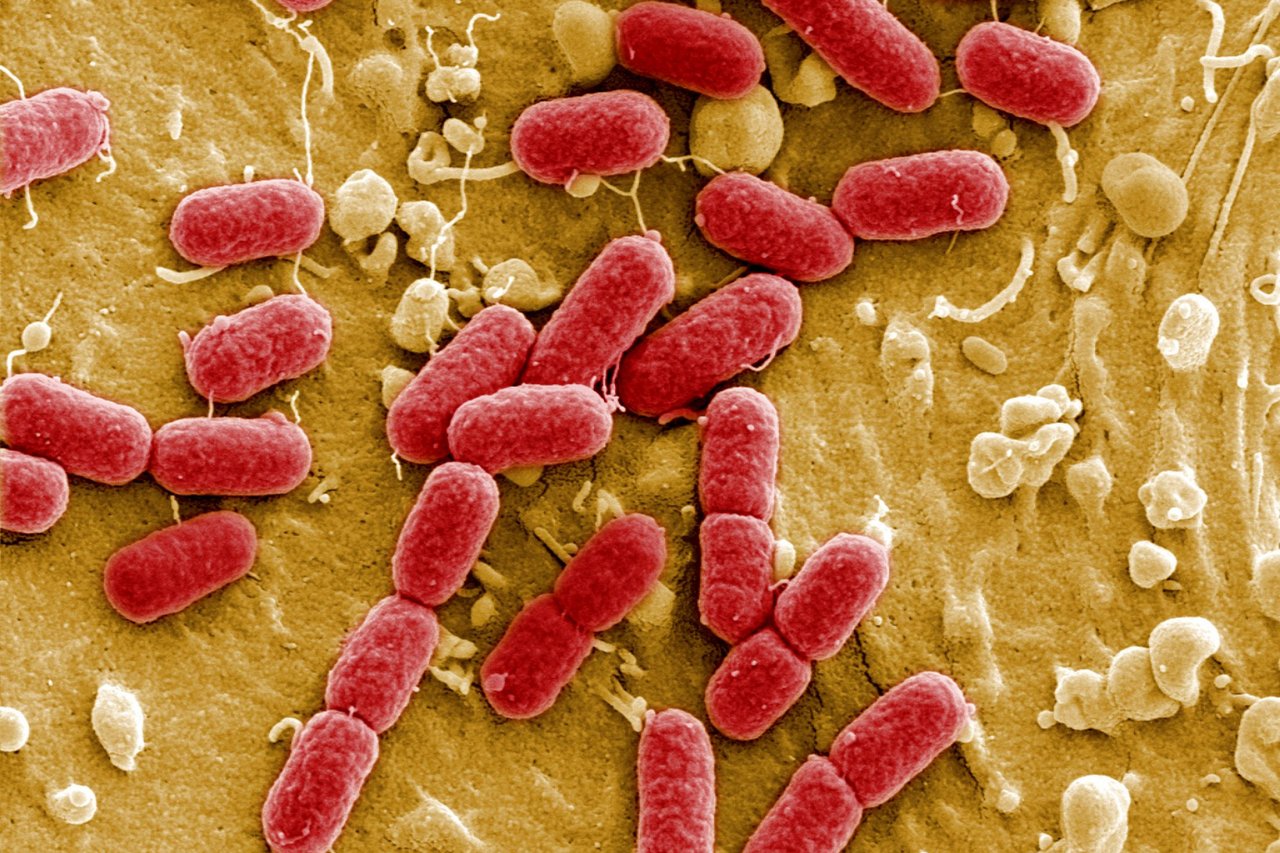
To investigate the prevalence of MDR bacteria among children, researchers from Case Western Reserve University School of Medicine studied patient data from 48 children's hospitals across the country. Using diagnostic and billing claim codes, they identified diagnoses of infections with Enterobacteriaceae, a bacterial family that includes salmonella, Escherichia coli and Shigella, among many others. And among these diagnoses, they singled out those that were categorized as multi-drug resistant.
Among approximately 107,000 diagnoses of Enterobacteriaceae infections in the hospital records they examined, the researchers found 724 instances of multi-drug resistance. That's just one percent of the infections resistant to antibiotics, but the eight-year span of the study, published this month in the Journal of the Pediatric Infectious Diseases Society, reveals a shocking trend. Although the total number of Enterobacteriaceae infections was fairly stable year to year, the proportion of these infections that were resistant to antibiotics rose from 0.2 percent in 2007 to 1.5 percent in 2015. "For the general public, the change from 0.2 to 1.5 percent may not mean a lot," says pediatrician and epidemiologist Sharon Meropol, who was lead author of the study. "But for infectious disease experts, it's ominous."
Further examination of the hospital records revealed additional disturbing facts. Most of the MDR infections were present in the children before they arrived at the hospital, which means an increasing amount of superbugs are circulating in U.S. communities. And although the analysis did not show a dramatically higher death rate among the superbug-infected children, there were more deaths in this group. Hospital stays were an average of four days longer (21 days versus 17 days) for the MDR infections compared with more easily treated Enterobacteriaceae infections. Older children and those with other illnesses were the most at risk for antibiotic-resistant illnesses.
The study has some possible weaknesses. Because the MDR infection count relied on diagnostic codes and billing claims from health care records, rather than blood samples or other biological data, the total may be inaccurate, says Michael Smith, who specializes in pediatric infectious diseases at the University of Louisville School of Medicine.
Improvements in tests for detecting MDR bacteria during the eight years covered by the study could have led to more diagnoses during the latter years, which "may have biased the reporting," says Janet Haas, director of epidemiology at Lenox Hill Hospital in New York. "Some caution in interpreting the data is warranted," says Haas.
Still, Smith and Haas agree that the trend is concerning. "The rate at which these discharges are increasing is very steep," says Haas. Smith also points out the parallel increase in superbugs from other bacterial families, such as methicillin-resistant Staphylococcus aureus, or MRSA, which causes a range of serious illnesses including pneumonia. And considering that the study focused on just 48 pediatric hospitals, the number of MDR infections among U.S. children could be much higher.
Experts largely trace the advent of superbugs to overuse of antibiotics. According to the Centers for Disease Control & Prevention, at least 30 percent of antibiotics prescribed each year in the U.S. are unnecessary. The excess presence of antibiotics enables the proliferations of bacterial strains that can withstand these treatments. As a result, a urinary tract infection caused by E. coli that was once easily eliminated with penicillin or cephalosporin now stubbornly persists despite rounds of these antibiotics. Administering antibiotics to livestock to make them grow faster and stay healthy—a practice that accounts for 80 percent of antibiotic use in the U.S.—also drives the superbug proliferation.
The ramifications of MDR infections are dire. Haas notes that when first- and second-line antibiotics have failed, some of the "drugs of last resort" may not be safe for children. The paucity of effective medications is leading some companies to reach for antibiotics shelved long ago because they were once considered too toxic. And as the findings of this new study show, the problem is escalating. "It is scary," says Meropol. "Infectious disease doctors are scared."
So are global public health authorities. This week, the World Health Organization published a list of "priority pathogens"—bacteria families with severe and dangerous antibiotic resistance—for the first time. Those considered the most urgent threats, including the Enterobacteriaceae family, are responsible for serious, sometimes fatal, infections arising in hospitals and nursing homes. These bacteria, like others on the WHO list, are known as "gram-negative," a term applied to bacterial pathogens containing internal structures that facilitate drug resistance as well as the ability to transfer that resistance genetically to other bacteria.
Meropol is optimistic about the possibility of halting or even reversing the trend. Dramatically reducing both the use of antibiotics in livestock and unwarranted prescriptions for humans could slow the spread of superbugs. Measures toward these ends are underway, such as the new rules issued by the U.S. Food and Drug Administration to control agricultural antibiotic use. Proactive prevention of bacterial illnesses—whether through the use of vaccines or simply improved hygiene—could also curtail the spread of superbugs, says Meropol. And, says Smith, physicians must do their part to stop overuse. "If you don't have compelling evidence for a bacterial infection," says Smith, "you should not prescribe antibiotics."
For the authors, the findings are a warning sign that must be heeded. "We must be vigilant," they write in their study, "and do everything possible to curtail and even reverse this process."