At the spanking new, ultra-modern Royal London Hospital in east London, an 11-year-old girl swathed in blue drapes is lying anaesthetised on an operating table. Consultant surgeon Kay Seymour gently re-ties the patient's blonde ponytail so it's out of the way. The girl's head is turned to the side so that just her ear is exposed. "Crocodile forceps please," says senior registrar Mahmood Bhutta, the ear, nose and throat surgeon who will carry out today's procedure. And so the operation begins.
Over the next 90 minutes, peering intently down a microscope into the ear canal, Bhutta deploys a range of exceedingly delicate, fine-ended stainless steel instruments to cut, scrape and effect a "scaffold" of cartilage to repair his patient's ear drum and snip away potentially dangerous skin growth. "A bit of extra skin doesn't sound that serious, but if it's left, it would carry on growing, eventually into her brain. It can kill," he explains. When the two surgeons are satisfied with the result, the girl is wheeled out to recovery. Her mum and dad, waiting at her bedside on the ward, look overcome with relief when they're told the operation has gone well. It's a young life saved.
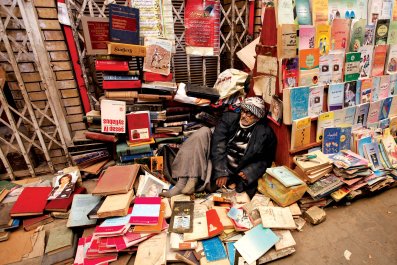
Fast forward a month. It's late October last year, and Mahmood Bhutta is wandering the back streets of Sialkot in north-east Pakistan. This is the city where his parents grew up, and it was from here that they emigrated to the UK in the 1970s. Sialkot is also the global centre of surgical instrument manufacture – around 80% of the world's supply is made here, and then shipped internationally.
Bhutta's tour of this not-so-smart neighbourhood of Sialkot comprised numerous meetings with surgical instrument factory owners. They were keen to offer him the reassurances he was seeking that labour standards had vastly improved on the poor conditions he found in his 2008 report for the British Medical Association on conditions at a range of factories in the city.
Despite these reassurances and years of campaigning via the BMA's Medical Fair and Ethical Trade Group, which he founded seven years ago, Bhutta's subsequent tour of the backstreets confirmed there were still very young children working in filthy, dangerous workshops to make the instruments he and his colleagues use every day in NHS operating theatres.

There are thousands of such small, unregulated units in Sialkot – they are "like open garages, the size of a medium-sized bedrooom" Bhutta explains – which are subcontracted by larger factories to make the component parts that will later be "finished" and assembled into surgical instruments ready for export.
And no matter how much better the working conditions inside those larger factories – Bhutta says that the improvements since his last visit to Sialkot have been considerable, partly because international medical supplies companies have demanded them – in these small subcontracted units, little if any progress appears to have been made.
"They're open to the street, you can easily look inside; we found a seven-year-old working on a grinding machine," says Bhutta. "We interviewed his dad – the boy started six months ago and works 11 hours a day. He gets occasional cuts and abrasions. And his dad told us he hates the work. He gets paid 4,000 rupees a month [a third of the adult minimum wage]. And he doesn't go to school any more."
The boy's 10-year-old brother also works in the unit. "The story is these kids' uncle died and there was family debt, and the dad had to take them out of school to work to pay it back," says Bhutta.
Theo Jaekel, a researcher from the independent Swedish watchdog organisation Swedwatch, who accompanied Bhutta on this trip, confirms that their party observed child labour in several small workshops. "In one case the manager denied that the child was working there," Jaekel recalls. "He said he was a neighbour's son who liked hanging round, but it was obvious he had a job. He was picking things up in the right order, putting them in cases, taking them to another worker."
The workshops are hazardous to adult workers, let alone for children, Jaekel says. "Dirty, with poor or no lighting, cramped rooms, and no safety equipment whatsoever – no breathing masks, goggles or ear plugs. The sound is deafening when you have all these grinding and polishing machines working, and a huge generator in the room so you can't even speak."
The risk of injury is ever-present. The loss of health is devastating to any impoverished individual when an employer does not pay for medical treatment or ongoing sick leave. These benefits are now provided – though typically informally, rather than contractually – in the bigger factories. But not here.
"Several workers told us that a recurring event is a grinding wheel coming off at full speed," says Jaekel. "They told us of injuries, and in this type of workplace they don't get help. One man told us of a friend who'd had a grinding wheel that flew off the machine and into his head."
This can kill. The man was lucky, though he'll never be able to work again.
International labour standards recognise that in some developing countries, impoverished families will rely on income earned by their children. It is stipulated, however, that children under 13 should not work, that hours must be limited, that children must be able to go to school and that the work cannot be carried out in hazardous conditions. Surgical instrument manufacture is inherently hazardous. So children should not be working in this sector at all.
More dangerous still, however, is the manufacture of the steel from which every pair of crocodile forceps and iris scissors, every scalpel, every suture needle – every surgical instrument laid out on trays in operating theatres across the world are made. Factories in Sialkot mostly source their steel from the forges in the nearby city of Daska. It's here, Bhutta says, that children may be at the most serious risk: child labour is rife in Daska's forges, where molten metal and forging hammers are ever-present dangers.
The UK spends £40bn a year on medical supplies, of which £5m goes on surgical instruments. There are issues with labour standards in various other product sectors: poor conditions in the manufacture of latex gloves were detailed in a report released last March by the Finnish watchdog FinnWatch. Swedwatch has recently made criticisms of how a manufacturer of theatre gowns treated its workers.
The UK government has no requirement for the NHS to source medical supplies based on ethical principles – a failure that Bhutta deplores. The BMA's Medical Fair and Ethical Trade Group has worked tirelessly to improve awareness of the need for better standards: in May it published its most recent set of guidelines for doctors working in general practice and healthcare commissioners. These are entirely voluntary, however: they have no teeth.
Bhutta believes that more radical measures need to be taken, and is now demanding that the government embeds internationally recognised principles of ethical trade and fair working conditions into the NHS's constitution. "The Department of Health is broadly supportive, but apparently they can't put this into policy," he says. "My opinion is that it's now time for ministers to stand up and say our NHS is going to support ethical procurement."
It looks like this commitment may be a long time coming, however: the most recent government document on the NHS's buying policies, called Better Procurement, Better Value, Better Care, was published in August 2013, and focuses solely on ways to save money. But endlessly driving the price down only exacerbates the problems for anyone trying to improve conditions in developing countries. And declaring loudly that the NHS is the biggest national healthcare system in the world doesn't cut it any more. At one of the largest factories Bhutta visited in Sialkot, the manager told him frankly that many companies including his own were no longer particularly interested in supplying the NHS, "because they get paid so little for it now. And then, he said, 'You're demanding all these conditions, but the prices keep falling'."
Even in the face of fierce competition, with determination and commitment, it is possible to transform working practices: 26-year-old Awais Asif is the proof. An MA student in Germany whose family lives in Sialkot, he put his studies on hold for two years to set up Abarut Industries, a small surgical instrument manufacturing unit, in partnership with his father.

With no experience in the sector but driven by horror at the working conditions he'd observed, the aim was to build his business as a model for how others might operate. It's been tough, he laughs. There were no customers for a very long time, only a large hole into which his father poured money. But workers are paid minimum wage, they are fed, their salaries are not subject to deductions if they're sick. He is investigating the possibility of a proper sickness insurance scheme, now he has some customers and turnover has improved.
Only one customer, Swansea-based DTR Medical, has ever asked him for any assurances on labour standards, via a faxed Q&A which he filled in and sent back. They've not followed it up with any checking, and have never visited his facility. His other customers in Poland, Saudi Arabia and Russia have never asked about labour conditions – only about quality and price. "Especially for our Russian customers, they do not understand," he says. "They ask, 'Why do you do so much?' So I don't talk so much about it to them."
Asif has gone into the business to make a change. But many others won't do it until they are pushed. The problems inherent in many medical supply chains were acknowledged in 2012 by the biggest single supplier of products to the NHS, Derbyshire-based company NHS Supply Chain, when it launched its own Labour Standards Assurance System (LSAS). Two years on, Stephanie Gibney, ethical and sustainability manager, says that in the two areas initially piloted – surgical instruments and medical textiles – 80 suppliers became contractually obliged to engage in a programme of constant improvement.
There may well be precious little difference to be seen as yet. On-the-ground checks are fundamental to the way that Fairtrade Foundation accredits companies in the coffee, tea, chocolate, cotton, fruit and flower industries, for example. Do the LSAS standards mean that suppliers to the NHS must physically go out to countries like Pakistan to see if what their suppliers are telling them about adherence to codes of conduct is true? It appears not.
An independent, third party audit is required, Gibney says, but not for the whole supply chain. Nobody is following a pair of crocodile forceps back from a UK supplier to the packaging plant which sterilised and packaged them, to the Pakistani factory before that which did the final finishing, or to the subcontracted unit on a Sialkot backstreet which made the component parts – or indeed to the Daska forge which produced the steel. "It's a progressive approach, so at the earlier stages, it's [about looking at] the supplier's direct operations, then it will start to look beyond that," Gibney says when pressed. "We're not ruling out audit – because audit can be incredibly positive . . . [but] because supply chains are quite long and complex there isn't a 'quick fix'."
At the Ethical Trading Initiative, director Peter McAllister is scathing of this response: companies that bemoan the complexity of their supply chains are failing to take their responsibilities seriously, he suggests.
"Those responses are way behind the curve," he says. "Extended supply chains are a fact of life. With the recent prawn scandal, for instance, it was about the conditions on the ships, where the waste from the fishing is what produces the feed that then supplies the prawn farms. It's not good enough to say 'It's very difficult'."
After suffering from labour standards scandals of its own, sports giant Nike, McAllister points out, put its whole supply chain into the public domain. He recently attended a meeting with the international fashion brand H&M which has done the same. "That's pretty brave. But their attitude now is 'Why should we want to hide problems? We want to know about the problems'."
The best companies, he says, "are not sitting there in London saying, 'This is difficult.' They're getting out out there, not hiding behind a code of conduct. I would argue that if you know there's a governance issue [in the country you're buying from], you should be working three times as hard."
In Pakistan, Bhutta believes, there are the beginnings of change – a growing understanding that children are entitled to an education, coupled with some international pressure to improve, mixed in with fear of a major scandal such as that which saw Nike pull out of its contract with Saga Sport in 2006 when child labour was found to be used in the making of footballs: the result was that a major Sialkot business collapsed. But pressure has to come from within, from the Pakistani government, and local business leaders too.
Conditions at big surgical instrument factories in Sialkot now are good by labour standards in Pakistan. Employees get the minimum wage, sick pay, receive care if they're injured, protective equipment is supplied. But it's estimated that two thirds of all the work in this industry is contracted out to small, unregulated workshops.
"Social requirements do have an effect, and that's an important message to take back," argues Jaekel. "And it's beyond just us saying 'Get safety goggles' and they get them. It's that they are now wanting to work with us and they understand why it's important." But, as Jaekel points out, it is largely an issue of resources. "Everyone said pricing is an issue. Prices have gone down, and if they don't get paid enough, they can't pay higher wages or improve the environment or increase safety. That needs to be transmitted back to the buyers in Europe."
"There is some evidence that what we and others are doing is making a difference, but I can tell you when I saw that seven-year-old I was still very saddened," says Bhutta. "There is no way you can sit back and say this job is done."
A seven-year-old boy who operates a grinding machine with no safety protection, and doesn't go to school. His 10-year-old brother. Their father, who like thousands of other surgical instrument workers is not paid the legal minimum wage. The man injured by an unguarded grinding wheel who can no longer work. His family for whom he can no longer provide. These people are the human cost of healthcare.
In London, Bhutta's 11-year-old patient has recovered from her operation. She's back at school, doing well.